

Table of Contents
- Quick Facts
- What Is Pancreatic Cancer?
- What Does the Pancreas Do?
- Types of Pancreatic Cancer
- Symptoms of Pancreatic Cancer
- Symptoms in Women
- When to See a Doctor
- Causes and Risk Factors
- Is Pancreatic Cancer Genetic?
- How Is Pancreatic Cancer Diagnosed?
- Pancreatic Cancer Stages
- Survival Rates and Prognosis
- Why Is Pancreatic Cancer So Deadly?
- Treatment Options
- Pancreatic Cancer Breakthrough and Emerging Treatments
- Prevention
- Living With Pancreatic Cancer
- Myths vs. Facts
- FAQ: Pancreatic Cancer
- Key Takeaways
Quick Facts
- Pancreatic cancer accounts for about 3% of all cancers in the United States but nearly 8% of all cancer deaths.
- Most people (around 80–85%) are diagnosed at an advanced stage, when the cancer has already spread.
- The five-year survival rate for all stages combined is approximately 13%.
- Pancreatic ductal adenocarcinoma (PDAC) is the most common type, making up around 90% of cases.
- Early-stage surgical removal gives patients the best chance of long-term survival.
- Several new drug therapies and targeted treatments are showing meaningful promise in clinical trials.
What Is Pancreatic Cancer?
Pancreatic cancer occurs when cells in the pancreas begin to grow and divide abnormally, forming a tumor. Over time, these cells can invade nearby tissues and spread to other organs — a process called metastasis.
What makes this cancer particularly challenging is how long it tends to develop silently. The pancreas sits deep in the abdomen, tucked behind the stomach, which means tumors rarely cause noticeable symptoms in their early stages. By the time most people receive a diagnosis, the cancer has often already reached an advanced stage.
Despite being less common than lung, breast, or colorectal cancer, pancreatic cancer carries a disproportionately high mortality rate — one of the highest among all major cancer types.
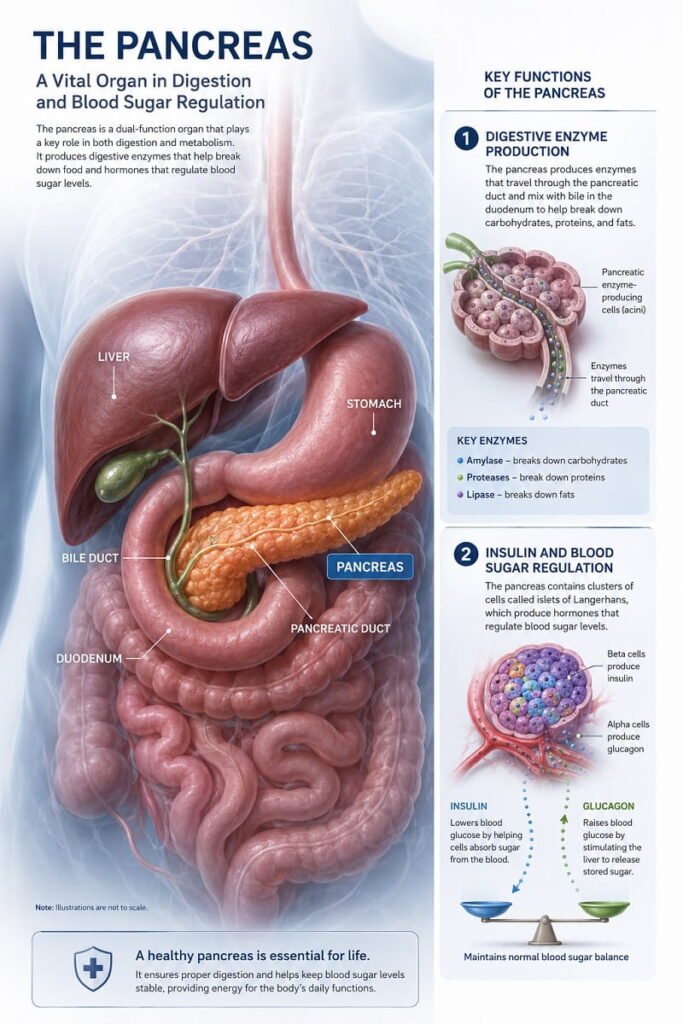
What Does the Pancreas Do?
The pancreas is a soft, oblong gland, roughly 15–25 centimeters long, located in the upper abdomen behind the stomach. It plays two major roles in the body:
Exocrine function: The pancreas produces digestive enzymes — including lipase, amylase, and protease — that are released into the small intestine to help break down fats, carbohydrates, and proteins.
Endocrine function: Clusters of cells called islets of Langerhans produce hormones, most critically insulin and glucagon, which regulate blood sugar levels.
Understanding these two functions matters when discussing cancer, because tumors arising from each cell type behave very differently.
Types of Pancreatic Cancer
Pancreatic Ductal Adenocarcinoma (PDAC)
This is by far the most common form, accounting for roughly 90% of all pancreatic cancers. It starts in the cells lining the pancreatic duct — the tube that carries digestive enzymes into the small intestine. PDAC is aggressive and tends to spread early, which partly explains why it’s so difficult to treat.
Pancreatic Neuroendocrine Tumors (PNETs)
Also called islet cell tumors or endocrine pancreatic cancer, PNETs arise from the hormone-producing cells of the pancreas. They are far less common (accounting for about 1–2% of pancreatic cancers) but are generally less aggressive than PDAC and carry a better prognosis.
PNETs can be:
- Functional — they produce hormones and cause symptoms related to hormone excess (such as low blood sugar or stomach ulcers).
- Non-functional — they don’t produce active hormones, and symptoms often come from tumor growth alone.
Notable cases such as Steve Jobs, who had a PNET, have raised public awareness of this rarer subtype.
Other Rare Types
- Acinar cell carcinoma — arises from enzyme-producing cells
- Solid pseudopapillary neoplasm — typically affects younger women and carries a good prognosis
- Pancreatoblastoma — rare, mainly occurs in children
| Type | Frequency | Aggressiveness | Prognosis |
|---|---|---|---|
| Pancreatic ductal adenocarcinoma | ~90% | Very high | Poor (if advanced) |
| Pancreatic neuroendocrine tumors | ~1–2% | Low to moderate | Better than PDAC |
| Acinar cell carcinoma | <2% | Moderate | Varies |
| Other rare types | <5% | Varies | Varies |
Symptoms of Pancreatic Cancer
What Are the Symptoms of Pancreatic Cancer?
Pancreatic cancer often causes no symptoms until it has grown significantly or spread. When symptoms do appear, they may include jaundice, unexplained weight loss, upper abdominal pain radiating to the back, new-onset diabetes, loss of appetite, pale or greasy stools, and dark urine. These symptoms are easy to overlook or attribute to other conditions.
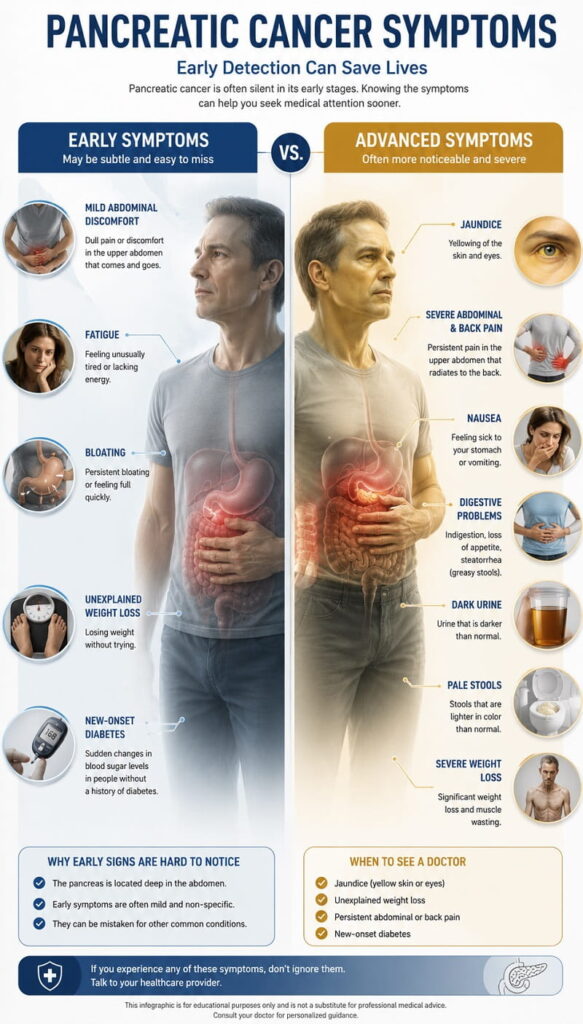
Early Symptoms
Early-stage pancreatic cancer rarely causes obvious symptoms, which is one of the main reasons it’s so often caught late. When early signs do occur, they tend to be vague and easy to dismiss:
- Mild, intermittent upper abdominal discomfort
- Subtle changes in digestion, such as bloating or feeling full quickly
- Unexplained fatigue
- A new diagnosis of diabetes with no clear cause (especially in people over 50 with no family history)
- Unexplained weight loss of more than a few pounds
Advanced Symptoms
As the cancer grows and potentially spreads, symptoms become more apparent and severe:
- Jaundice: Yellowing of the skin and whites of the eyes. This occurs when a tumor blocks the bile duct, causing bile to build up in the bloodstream. It is often one of the first symptoms people notice.
- Dark urine and pale stools: Both are caused by the same bile duct obstruction that produces jaundice.
- Persistent abdominal or back pain: A dull ache in the upper abdomen that radiates to the mid or lower back is a hallmark symptom, often worsening when lying flat.
- Severe weight loss and loss of appetite: Driven by both the cancer itself and impaired digestion.
- Nausea and vomiting: Particularly when the tumor affects the stomach outlet.
- New or worsening diabetes: The tumor can damage the insulin-producing cells, destabilizing blood sugar.
- Blood clots (deep vein thrombosis): Pancreatic cancer increases clotting risk.
- Itchy skin: Related to bile salt buildup from jaundice.
Digestive Symptoms
Because the pancreas is central to digestion, many symptoms relate to how food is processed. Patients may notice:
- Greasy, foul-smelling stools that float (called steatorrhea)
- Diarrhea or constipation
- Bloating and gas
- Difficulty digesting fatty foods
These symptoms arise when the tumor reduces the pancreas’s ability to produce digestive enzymes.
Symptoms in Women
Pancreatic cancer symptoms are broadly the same in men and women. However, some studies suggest women may be more likely to initially attribute symptoms like abdominal pain, bloating, and digestive changes to conditions such as irritable bowel syndrome (IBS) or menstrual-related issues, which can delay diagnosis.
Women should pay particular attention to:
- Unexplained weight loss alongside digestive changes
- New or worsening back pain with no clear orthopedic cause
- Jaundice appearing without a known liver condition
- A new diabetes diagnosis without family history or typical risk factors
There is no compelling evidence that pancreatic cancer presents fundamentally differently in women versus men, but awareness of these overlap risks is important.
When to See a Doctor
See a doctor promptly if you experience:
- Jaundice (yellow skin or eyes) — this always warrants urgent evaluation
- Unexplained weight loss of 5% or more of body weight over a few months
- Persistent upper abdominal pain, especially if it radiates to the back
- New-onset diabetes, particularly if you are over 50 and have no family history or typical risk factors
- Pale, greasy, or floating stools combined with dark urine
- Loss of appetite lasting more than two weeks
None of these symptoms definitively mean pancreatic cancer — many have benign explanations — but they should always be investigated by a physician.
Causes and Risk Factors
No single cause has been identified for most cases of pancreatic cancer. Instead, multiple factors appear to increase the risk.
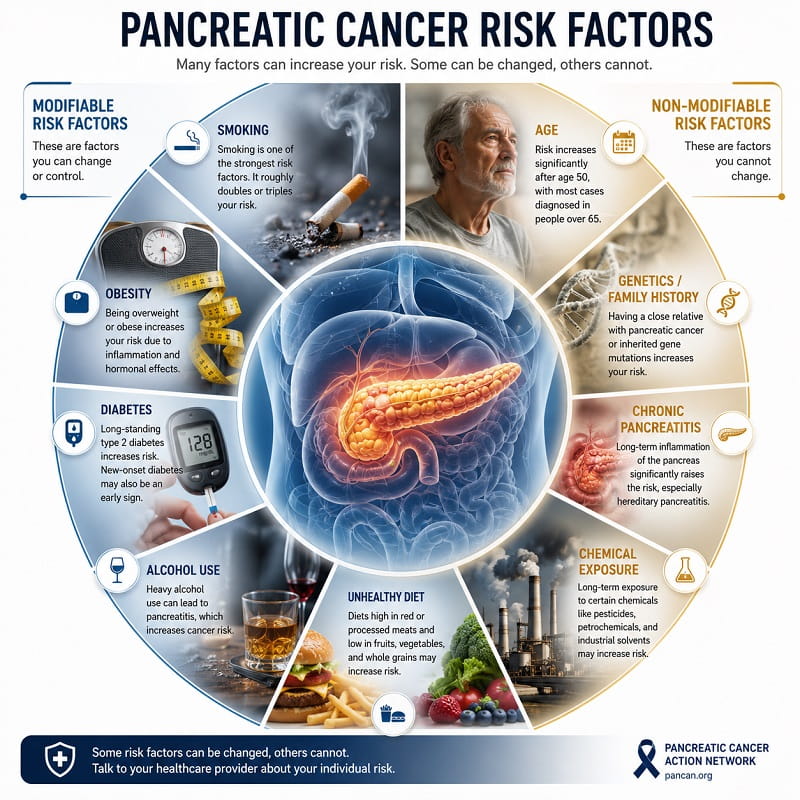
Smoking and Tobacco Use
Smoking is one of the strongest modifiable risk factors. Smokers are roughly two to three times more likely to develop pancreatic cancer than non-smokers. Tobacco carcinogens reach the pancreas through the bloodstream and bile duct. The risk decreases after quitting, though it remains elevated for years.
Obesity and Physical Inactivity
People with obesity (a body mass index over 30) have a 20–50% higher risk compared to those at a healthy weight. Excess fat, particularly around the abdomen, contributes to insulin resistance and chronic inflammation — both linked to cancer development.
Diabetes
There is a well-documented, bidirectional relationship between diabetes and pancreatic cancer. Long-standing type 2 diabetes is a modest risk factor. However, new-onset diabetes — particularly in people over 50 who suddenly develop it without typical risk factors — can sometimes be an early sign of a pancreatic tumor affecting insulin regulation.
Chronic Pancreatitis
Chronic pancreatitis (persistent inflammation of the pancreas) increases the risk of pancreatic cancer, especially when caused by hereditary mutations. Long-term alcohol-related pancreatitis also raises risk.
Age
Pancreatic cancer is rare before age 45. The majority of cases are diagnosed in people between 65 and 74. The risk increases significantly with age.
Alcohol
Heavy alcohol consumption raises the risk indirectly by contributing to chronic pancreatitis and liver disease, both of which are pancreatic cancer risk factors. Moderate drinking has not been shown to carry a significant risk.
Diet
Diets high in processed meats, red meats, and saturated fats may modestly increase risk. Conversely, diets rich in fruits, vegetables, and fiber are associated with lower risk, though evidence remains less definitive than for other risk factors.
Workplace Exposures
Prolonged exposure to certain chemicals — including pesticides, benzene, petrochemicals, and certain dyes — has been associated with a higher risk.
Risk Factor Summary
| Risk Factor | Level of Evidence | Relative Risk Increase |
|---|---|---|
| Smoking | Strong | 2–3× |
| Hereditary gene mutations | Strong | Up to 10× or more |
| Chronic pancreatitis | Strong | 13–18× (hereditary type) |
| New-onset diabetes (age 50+) | Strong | ~8× |
| Obesity | Moderate | 1.2–1.5× |
| Heavy alcohol use | Moderate | Indirect (via pancreatitis) |
| Diet (processed meats) | Modest | 1.1–1.3× |
Is Pancreatic Cancer Genetic?
About 10% of pancreatic cancers are linked to inherited gene mutations — meaning they run in families. Understanding this matters because close relatives of affected individuals may qualify for genetic screening and surveillance programs.
Key Genes Associated With Increased Risk
- BRCA1 and BRCA2: Most commonly associated with breast and ovarian cancer, but BRCA2 mutations in particular carry a significantly elevated pancreatic cancer risk.
- PALB2: Another gene associated with breast cancer that also increases pancreatic risk.
- ATM: Mutations in this DNA repair gene raise risk.
- CDKN2A (p16): Strongly linked to familial pancreatic cancer and also associated with melanoma.
- STK11 (Peutz-Jeghers syndrome): This condition carries one of the highest lifetime risks for pancreatic cancer.
- Lynch syndrome genes (MLH1, MSH2, MSH6, PMS2): Primarily known for colorectal and endometrial cancer, but pancreatic cancer risk is also elevated.
- PRSS1: Associated with hereditary pancreatitis, which significantly elevates lifetime risk.
Should You Get Genetic Testing?
Genetic testing is recommended if you have:
- Two or more first-degree relatives with pancreatic cancer
- One first-degree relative diagnosed at a young age
- A known family mutation (such as BRCA2) that increases risk
- A personal diagnosis of pancreatic cancer (to guide treatment decisions, particularly for PARP inhibitor eligibility)
Genetic counseling before and after testing is strongly recommended to help interpret results and make informed decisions.
How Is Pancreatic Cancer Diagnosed?
Imaging Tests
CT scan (computed tomography): The most commonly used first-line imaging tool. It can identify tumors, show their size and location, and reveal whether they have spread to nearby blood vessels or organs.
MRI (magnetic resonance imaging): Particularly useful for examining the bile duct and liver in detail. MRCP (magnetic resonance cholangiopancreatography) is a specialized MRI sequence that produces detailed images of the pancreatic and bile ducts.
PET scan: Used to detect cancer spread in distant parts of the body. Typically used for staging rather than initial diagnosis.
Ultrasound: Abdominal ultrasound is usually the first test when jaundice appears, to look for bile duct obstruction.
Endoscopic Procedures
Endoscopic ultrasound (EUS): A thin flexible tube with an ultrasound probe is passed through the mouth into the stomach, allowing very close imaging of the pancreas from inside the digestive tract. This provides much finer detail than external ultrasound. EUS can also guide a biopsy needle with high precision.
ERCP (endoscopic retrograde cholangiopancreatography): Used to visualize the bile and pancreatic ducts, and to place a stent if a duct is blocked — relieving jaundice.
Blood Tests
CA 19-9 (cancer antigen 19-9): This is the most widely used tumor marker for pancreatic cancer. Elevated CA 19-9 levels can suggest the presence of a pancreatic tumor, but it is not specific — levels can be raised in pancreatitis, bile duct conditions, and other cancers. CA 19-9 is most useful for monitoring treatment response rather than initial diagnosis. Notably, about 5–10% of people cannot produce CA 19-9 at all (a blood group variation), making the test unhelpful in those individuals.
CEA (carcinoembryonic antigen): Another tumor marker, less specific but sometimes elevated in pancreatic cancer.
Liver function tests: Elevated bilirubin and liver enzymes can point to bile duct obstruction.
Complete blood count and metabolic panel: General markers to assess overall health.
Biopsy
A tissue biopsy — removing a small sample of tumor cells — is needed to confirm the diagnosis. This can be done via:
- EUS-guided fine needle aspiration (FNA) or biopsy (FNB): Most commonly used.
- CT-guided biopsy: When EUS is not available or the tumor is in a difficult location.
- Surgical biopsy: Sometimes obtained during surgery itself.
Molecular profiling of the biopsy sample is increasingly important, as it helps identify specific genetic mutations that may respond to targeted therapies.
Pancreatic Cancer Stages
Staging describes how far the cancer has spread and guides treatment decisions. The most commonly used system is the TNM system (Tumor, Node, Metastasis), which is grouped into Stages 1 through 4.
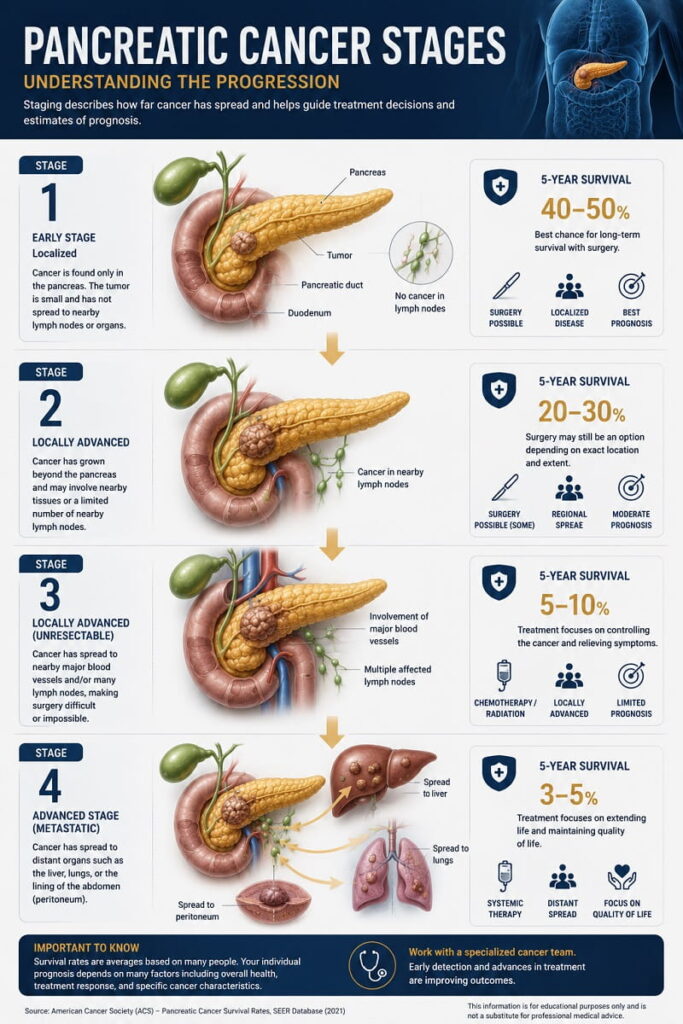
Stage 1
The tumor is confined entirely to the pancreas:
- Stage 1A: Tumor is 2 cm or smaller
- Stage 1B: Tumor is between 2 and 4 cm
At this stage, the cancer has not spread to nearby lymph nodes or distant organs. Surgery is usually possible and gives the best outcomes.
Stage 2
The tumor has grown beyond the pancreas but has not reached major blood vessels. It may or may not have spread to a small number of nearby lymph nodes.
- Surgery may still be possible at Stage 2A (no lymph node involvement).
- At Stage 2B, with limited lymph node involvement, surgery is often still considered if the tumor can be fully removed.
Stage 3
The cancer has spread to nearby major blood vessels (such as the superior mesenteric artery or celiac axis) and/or more lymph nodes. At this stage:
- Surgery is often no longer possible because removing the tumor would require removing critical blood vessels.
- This stage is often described as “locally advanced” or “unresectable.”
- Treatment typically focuses on chemotherapy, radiation, or a combination.
Stage 4
The cancer has spread to distant organs, most commonly the liver, lungs, or peritoneum (the lining of the abdominal cavity). This is called metastatic pancreatic cancer.
- Stage 4 is considered incurable with current standard treatments.
- Treatment goals shift toward controlling the cancer, managing symptoms, and maintaining quality of life as long as possible.
- Approximately 50–55% of all pancreatic cancer diagnoses are made at Stage 4.
Terminal Pancreatic Cancer
“Terminal” typically refers to Stage 4 disease that is no longer responding to treatment, where the focus has fully shifted to comfort-focused palliative care. This is a deeply difficult stage for patients and families, and specialized palliative care teams play a crucial role in supporting physical comfort, emotional wellbeing, and dignity.
Stage Overview Table
| Stage | Description | Surgery Possible? | 5-Year Survival |
|---|---|---|---|
| Stage 1 | Confined to pancreas | Usually yes | ~40–50% |
| Stage 2 | Beyond pancreas, no major vessels | Often yes | ~20–30% |
| Stage 3 | Involves major blood vessels | Rarely | ~5–10% |
| Stage 4 | Spread to distant organs | No | ~3–5% |
Survival figures are approximate population averages; individual outcomes vary significantly.
Survival Rates and Prognosis
Understanding Survival Statistics
Survival rates are calculated from population-level data and represent the percentage of people who are alive a certain number of years after diagnosis. They are meaningful at the population level but cannot predict what will happen to any individual patient.
The most commonly cited figure — the five-year relative survival rate — compares survival in people with pancreatic cancer to that of the general population of similar age.
Current Survival Rate Data
| Stage at Diagnosis | 5-Year Relative Survival Rate |
|---|---|
| Localized (Stage 1–2) | ~44% |
| Regional (Stage 3) | ~15% |
| Distant (Stage 4) | ~3% |
| All stages combined | ~13% |
Source: American Cancer Society, SEER Database data (most recent available)
These numbers represent averages from patients diagnosed several years ago. Current patients treated with newer drug combinations may do somewhat better, and clinical trial data continues to improve.
Can You Survive Stage 4 Pancreatic Cancer?
Stage 4 pancreatic cancer is not curable with standard treatments. However, some patients do live significantly longer than statistics suggest. Factors that influence prognosis include overall health, response to treatment, access to clinical trials, and specific tumor genetics.
There are documented cases of individuals living three, five, or even more years with Stage 4 disease — but these remain uncommon. Treatment decisions should be made with oncologists who specialize in pancreatic cancer, ideally at high-volume cancer centers where the full range of therapies, including clinical trials, is available.
Why Prognosis Has Improved (But Remains Challenging)
The five-year survival rate for pancreatic cancer has improved over the past decade — from around 6–7% to approximately 13% — largely due to more effective chemotherapy combinations such as FOLFIRINOX and gemcitabine plus nab-paclitaxel (Abraxane). Improvements in surgical technique and better patient selection for surgery have also contributed.
Despite this progress, pancreatic cancer remains one of the most difficult cancers to treat.
Why Is Pancreatic Cancer So Deadly?
Several interconnected factors explain why pancreatic cancer has such a poor prognosis:
1. Silent early development. Tumors grow without producing symptoms for months or years. By the time symptoms appear, the cancer is usually advanced.
2. Deep anatomical location. The pancreas is surrounded by critical blood vessels, the stomach, liver, and duodenum. Tumors often wrap around or invade these structures early, making surgery technically challenging or impossible.
3. Rapid spread. Pancreatic cancer cells often shed into the bloodstream and lymphatic system very early — sometimes even before a tumor reaches a detectable size.
4. Dense tumor environment (stroma). Pancreatic tumors are surrounded by a thick, fibrous tissue layer called the tumor stroma. This creates a physical barrier that reduces blood flow to the tumor, making it harder for chemotherapy drugs to reach cancer cells.
5. High resistance to chemotherapy. Pancreatic cancer cells often develop mechanisms to pump out or neutralize chemotherapy drugs.
6. Lack of effective early screening. Unlike colon or breast cancer, there are no widely recommended blood tests or imaging protocols for screening the general population. Even among high-risk individuals, optimal screening approaches are still being refined.
7. Complex biology. The genetic and molecular diversity of pancreatic tumors means that what works for one patient may not work for another.
Treatment Options
Treatment depends on the stage of the cancer, its location, the patient’s overall health, and tumor genetics. A multidisciplinary team — including surgical oncologists, medical oncologists, radiation oncologists, gastroenterologists, and palliative care specialists — should be involved in decision-making.

Surgery
Surgery is the only potential cure for pancreatic cancer, but it is only possible in roughly 15–20% of patients at diagnosis — those whose tumors are confined to the pancreas or have not invaded major blood vessels.
Whipple procedure (pancreaticoduodenectomy): The most complex and most commonly performed operation. The surgeon removes the head of the pancreas, the duodenum, part of the stomach, the gallbladder, and nearby lymph nodes, then reconstructs the digestive tract. It is a major operation requiring significant recovery (typically 6–10 days in hospital) and is best performed at high-volume specialized centers where outcomes are demonstrably better.
Distal pancreatectomy: Removal of the body and tail of the pancreas, sometimes with the spleen. Used when tumors are located in the left side of the pancreas.
Total pancreatectomy: Removal of the entire pancreas. Required in some cases but leads to permanent diabetes and pancreatic insufficiency.
Minimally invasive (laparoscopic or robotic) approaches to these surgeries are increasingly available at specialized centers and may result in shorter recovery times.
Chemotherapy
Chemotherapy is the main treatment for patients who cannot have surgery (the majority) and is also used before surgery (neoadjuvant) to shrink tumors, or after surgery (adjuvant) to reduce recurrence risk.
Current standard regimens include:
- FOLFIRINOX (5-fluorouracil, leucovorin, irinotecan, oxaliplatin): A four-drug combination shown to be more effective than single-agent gemcitabine for patients who are healthy enough to tolerate it.
- Gemcitabine + nab-paclitaxel (Abraxane): A well-established combination that has improved survival compared to gemcitabine alone.
- Gemcitabine alone: Used in patients who cannot tolerate more intensive regimens.
- NALIRIFOX: A newer combination (nanoliposomal irinotecan + 5-fluorouracil + leucovorin + oxaliplatin) showing improved survival in first-line metastatic disease.
Radiation Therapy
Radiation uses high-energy beams to kill cancer cells or slow tumor growth. In pancreatic cancer, it is used primarily for:
- Locally advanced, unresectable tumors (Stage 3)
- After surgery to reduce recurrence risk (often combined with chemotherapy)
- Palliative symptom relief (such as pain control)
Techniques include conventional external beam radiation and stereotactic body radiation therapy (SBRT), which delivers precise, high-dose radiation in fewer sessions.
Targeted Therapy
Targeted therapies are drugs designed to attack specific molecular features of cancer cells, causing less damage to normal cells compared to standard chemotherapy.
Currently approved or widely used targeted therapies for pancreatic cancer include:
Erlotinib (Tarceva): Targets the EGFR (epidermal growth factor receptor) pathway. Modestly improves outcomes when combined with gemcitabine.
Olaparib (Lynparza): A PARP inhibitor approved for patients with a germline BRCA1 or BRCA2 mutation whose disease has not progressed during platinum-based chemotherapy. This was a significant milestone — the first targeted therapy for a genetically defined subset of pancreatic cancer patients.
This is precisely why molecular profiling of tumors at diagnosis has become increasingly standard — knowing a patient’s BRCA status or other genetic markers directly affects which treatments they may benefit from.
Immunotherapy
The immune system can, in principle, recognize and destroy cancer cells. Immunotherapy drugs help it do so more effectively. However, pancreatic cancer has proven largely resistant to immunotherapy, primarily because:
- The dense tumor stroma physically excludes immune cells.
- Pancreatic tumors have relatively few genetic mutations (“low tumor mutational burden”), making them less visible to the immune system.
- Pancreatic cancer creates an immunosuppressive environment around itself.
Pembrolizumab (Keytruda): Approved for any solid tumor (including pancreatic cancer) that is MSI-H (microsatellite instability-high) or has mismatch repair deficiency (dMMR). Only about 1–2% of pancreatic cancers carry this biomarker, but for those patients, pembrolizumab can be effective.
Research continues on combining immunotherapy with other treatments to overcome the cold tumor microenvironment of pancreatic cancer.
Palliative Procedures
Even when curative treatment is not possible, procedures can significantly improve quality of life:
- Biliary stenting: A small tube (stent) placed via ERCP to open a blocked bile duct and relieve jaundice.
- Celiac nerve block: An injection that can significantly reduce the severe abdominal and back pain associated with advanced disease.
- Gastric bypass: For tumors causing gastric outlet obstruction, a surgical bypass allows food to pass normally.
Pancreatic Cancer Breakthrough and Emerging Treatments
Pancreatic cancer research is moving faster than it has at any previous point, driven by a deeper understanding of the disease’s molecular biology.
KRAS-Targeted Therapies
KRAS mutations are found in approximately 90% of pancreatic adenocarcinomas, making KRAS the most important oncogene in this disease. For decades, KRAS was considered “undruggable.” That changed with the approval of sotorasib for KRAS G12C mutations in lung cancer — though the G12C mutation is rare in pancreatic cancer.
Daraxonrasib (RMC-6236): One of the most closely watched experimental drugs in pancreatic oncology, daraxonrasib is a next-generation RAS/MAPK inhibitor designed to broadly target multiple KRAS mutations — not just G12C. Early clinical trial data (presented at major oncology meetings through 2024) showed meaningful tumor shrinkage in patients with heavily pretreated pancreatic cancer. It is currently being evaluated in multiple trials, including as a first-line therapy. While it remains investigational, the early signals are considered genuinely promising by the oncology community.
Adagrasib and other KRAS G12D/G12V inhibitors: Additional compounds targeting the most common KRAS mutations in pancreatic cancer (G12D and G12V) are in active clinical development.
mRNA Vaccines
Building on mRNA technology developed during the COVID-19 pandemic, researchers are developing personalized cancer vaccines tailored to each patient’s tumor mutations. Early pancreatic cancer trials (including work from BioNTech and Memorial Sloan Kettering) showed encouraging results in a small cohort, with some patients generating sustained immune responses that appeared to delay recurrence. Larger trials are underway.
Antibody-Drug Conjugates (ADCs)
ADCs are precision-engineered molecules that combine a cancer-targeting antibody with a chemotherapy payload, delivering the drug directly to tumor cells. Several ADCs targeting proteins expressed on pancreatic cancer cells are in clinical trials.
Combination Approaches
Many investigators believe the path forward lies in combining multiple treatment types — for example, immunotherapy with targeted agents or vaccines, or chemotherapy with drugs that disrupt the tumor stroma to make cells more accessible.
Clinical Trials
For patients with advanced or recurrent pancreatic cancer, clinical trials may offer access to therapies not yet widely available. Major cancer centers — including MD Anderson, Memorial Sloan Kettering, Johns Hopkins, and others — often have multiple ongoing trials. Patients and families can search available trials at clinicaltrials.gov.
Prevention
There is no guaranteed way to prevent pancreatic cancer, but certain lifestyle choices meaningfully reduce risk.
Lifestyle Changes That Reduce Risk
- Stop smoking: If you smoke, quitting is the single most impactful modifiable step. The risk begins to fall within a few years of quitting.
- Maintain a healthy weight: Excess body fat, particularly abdominal fat, is a known risk factor. Gradual, sustainable weight management through diet and exercise helps.
- Limit alcohol: Heavy drinking contributes to pancreatitis, which in turn elevates cancer risk.
- Eat a plant-rich diet: Diets emphasizing fruits, vegetables, legumes, whole grains, and fiber — while limiting processed and red meats — are associated with lower risk.
- Exercise regularly: Physical activity reduces obesity risk and helps regulate insulin, both protective factors.
- Manage diabetes: Poorly controlled blood sugar may contribute to cancer risk over time.
Screening for High-Risk Individuals
For most people, routine pancreatic cancer screening is not currently recommended because the cancer is rare enough that population-wide screening would produce too many false positives without proven benefit.
However, screening may be recommended for people at significantly elevated risk, including:
- Those with two or more close relatives with pancreatic cancer
- Carriers of BRCA2, PALB2, ATM, CDKN2A, STK11, or Lynch syndrome mutations
- People with hereditary pancreatitis
When surveillance is recommended, it typically involves annual MRI/MRCP or endoscopic ultrasound (EUS), starting at age 50 (or 10 years younger than the youngest affected relative).
Referral to a specialized familial pancreatic cancer program at a major cancer center is advisable for those at high inherited risk.
Living With Pancreatic Cancer
A pancreatic cancer diagnosis is one of the most difficult things a person — and their family — can face. The physical, emotional, and practical challenges are immense. The following guidance is intended to support quality of life at every stage.
Nutrition
Because the pancreas is essential to digestion, patients often struggle with:
- Poor appetite
- Weight loss and muscle wasting (cachexia)
- Malabsorption of fats (leading to steatorrhea)
- Nausea
Pancreatic enzyme replacement therapy (PERT): Most patients with exocrine insufficiency benefit enormously from taking prescription enzyme supplements with meals. These replace the digestive enzymes the damaged pancreas can no longer produce adequately.
Working with an oncology dietitian is strongly recommended. Small, frequent meals; soft, easy-to-digest foods; and high-calorie, high-protein foods are generally encouraged.
Pain Management
Pain is one of the most distressing symptoms of advanced pancreatic cancer. Effective options include:
- Oral and IV pain medications: Including opioid analgesics when appropriate, titrated carefully for comfort.
- Celiac plexus neurolysis: A targeted nerve block that can dramatically reduce the severe back and abdominal pain caused by tumor pressure on the celiac nerve plexus. This can be performed endoscopically or under CT guidance.
- Radiation therapy for pain relief: Can shrink the tumor enough to reduce pressure on surrounding structures.
Patients should never feel they need to endure uncontrolled pain. Because palliative care specialists are expert at managing pain without necessarily hastening death.
Palliative Care
Palliative care is specialized medical care focused on relieving suffering and improving quality of life — for both patients and their families. It is not the same as hospice or “giving up.” Palliative care can and should be integrated from the time of diagnosis, alongside active treatment.
Palliative care teams help with:
- Symptom management (pain, nausea, fatigue, depression)
- Goals of care conversations
- Coordination across medical teams
- Support for family caregivers
- Planning for end-of-life care when needed
Research consistently shows that patients who receive early palliative care alongside treatment have better quality of life and — in some studies — even live longer.
Emotional Health
A cancer diagnosis brings fear, grief, anger, and uncertainty. These are completely normal responses. Psychological support may include:
- Individual therapy or counseling with a trained oncology social worker or psychologist
- Cancer support groups (in-person or online)
- Peer support programs (connecting with others who have the same diagnosis)
- Mindfulness-based stress reduction programs
- Family therapy to help loved ones cope
Organizations such as the Pancreatic Cancer Action Network (PanCAN) offer free emotional support and navigation resources.
Supporting a Loved One
For family members and caregivers:
- Ask the patient what kind of support they want — don’t assume.
- Help with practical tasks (meals, appointments, medications) without taking over.
- Accept help from others — caregiving is emotionally and physically exhausting.
- Seek your own support. Caregiver burnout is real, and looking after yourself is not selfish.
- Be present. Often what matters most is simply not being alone.
Myths vs. Facts
| Myth | Fact |
|---|---|
| Pancreatic cancer always runs in families | Only about 10% of cases are linked to inherited mutations. Most cases arise without a family history. |
| Pancreatic cancer always causes severe pain | Many early-stage cases cause little or no pain. Pain becomes more common as the cancer progresses. |
| If you have diabetes, you’ll get pancreatic cancer | Diabetes slightly increases risk, but the vast majority of people with diabetes do not develop pancreatic cancer. |
| Once diagnosed with pancreatic cancer, survival is measured in weeks | While prognosis is often poor, many patients live months to years, especially with early diagnosis and effective treatment. |
| Surgery is always an option | Surgery is only possible for roughly 15–20% of patients at the time of diagnosis. |
| Pancreatic cancer is always caused by lifestyle choices | Risk factors like obesity and smoking play a role, but many patients have no identifiable risk factors. |
| Immunotherapy doesn’t work for any pancreatic cancer patient | Pembrolizumab is effective for the small subset (1–2%) with MSI-H tumors. Research on broader immunotherapy is active. |
FAQ: Pancreatic Cancer
What is the most common early sign of pancreatic cancer?
The most common early signs — such as mild abdominal discomfort, subtle digestive changes, and unexplained weight loss — are vague and easily missed. Jaundice (yellowing of the skin) is often the first symptom that brings people to the doctor, but it more typically indicates the cancer is already advanced enough to block the bile duct.
Is pancreatic cancer curable?
Pancreatic cancer can be cured when caught early enough to be surgically removed — roughly in Stage 1 or early Stage 2. Unfortunately, the majority of patients are diagnosed at advanced stages where surgery is not possible. Research into earlier detection and more effective treatments is ongoing.
How is pancreatic cancer different from pancreatitis?
Pancreatitis is inflammation of the pancreas, usually caused by gallstones or alcohol. It is not cancer, though chronic pancreatitis is a risk factor for developing pancreatic cancer over time. The two conditions share some overlapping symptoms (abdominal pain, nausea, digestive issues), which sometimes complicates early diagnosis.
What is the Whipple procedure?
The Whipple procedure (pancreaticoduodenectomy) is a complex surgery to remove the head of the pancreas, duodenum, part of the stomach, gallbladder, and nearby lymph nodes. It is the most common surgery for pancreatic cancer located in the head of the pancreas and offers the best chance of cure for early-stage disease.
What does the CA 19-9 test show?
CA 19-9 is a protein (tumor marker) that is elevated in the blood of many pancreatic cancer patients. It is not a definitive diagnostic test — it can be elevated in other conditions too — but it is useful for monitoring treatment response and checking for recurrence.
Can pancreatic cancer be caught by a blood test?
Currently, no single blood test can reliably diagnose pancreatic cancer in its early stages. CA 19-9 lacks sufficient sensitivity and specificity for screening. Researchers are working on liquid biopsy tests (detecting cancer DNA or proteins in the blood) that may eventually allow for earlier detection, but these are not yet in routine clinical use.
What are pancreatic neuroendocrine tumors?
Pancreatic neuroendocrine tumors (PNETs) arise from the hormone-producing cells of the pancreas, not the ductal cells. They are generally less aggressive than pancreatic adenocarcinoma and carry a better prognosis. Steve Jobs, for example, was diagnosed with a PNET. They are relatively rare and may behave very differently from the more common PDAC.
Is pancreatic cancer related to diet?
Diet plays a modest role. Diets high in processed and red meats may slightly increase risk, while diets rich in vegetables, fruits, and fiber are associated with lower risk. Diet alone is unlikely to cause pancreatic cancer, but alongside other risk factors, it contributes to overall risk.
What stage is usually diagnosed?
Approximately 50–55% of pancreatic cancer cases are diagnosed at Stage 4 (metastatic), meaning the cancer has already spread to distant organs. Only about 10–15% are caught at an early, localized stage where surgery may be possible.
What new treatments are available?
Key advances include the NALIRIFOX regimen for first-line metastatic disease, the PARP inhibitor olaparib for BRCA-mutated tumors, and promising investigational drugs targeting KRAS mutations (including daraxonrasib). Personalized mRNA cancer vaccines and antibody-drug conjugates are in active clinical trials. Patients should ask their oncologist about available clinical trials.
Key Takeaways
- Pancreatic cancer is among the most serious cancers due to late diagnosis, rapid spread, and resistance to many treatments — but survival rates are gradually improving.
- The pancreas serves two vital roles: producing digestive enzymes and regulating blood sugar.
- Pancreatic ductal adenocarcinoma (PDAC) accounts for ~90% of cases. Pancreatic neuroendocrine tumors (PNETs) are rarer and generally less aggressive.
- Symptoms are often absent or vague in early disease. Jaundice, persistent back/abdominal pain, unexplained weight loss, and new-onset diabetes in older adults are key warning signs.
- About 10% of cases are linked to inherited gene mutations. High-risk individuals should discuss genetic testing and surveillance with a specialist.
- Surgery offers the only potential cure but is possible in only ~15–20% of patients.
- Chemotherapy regimens like FOLFIRINOX and gemcitabine + nab-paclitaxel are current first-line standards for most patients.
- Targeted therapy (olaparib) benefits the subset of patients with BRCA mutations.
- The KRAS pathway is now a major area of research, with drugs like daraxonrasib showing early promise.
- Early palliative care, pain management, nutritional support, and psychological care are essential parts of comprehensive treatment.
- Quitting smoking, maintaining a healthy weight, and eating a plant-rich diet are the most evidence-based prevention strategies.
- Clinical trials represent an important option for patients with advanced disease; major cancer centers offer the broadest access.
This article is intended for educational purposes and does not constitute medical advice. If you have concerns about pancreatic cancer symptoms or risk factors, please consult a qualified healthcare provider. Medical knowledge in this area is advancing rapidly; always seek current guidance from a board-certified oncologist or specialist.
Related Articles:



