
Featured Snippet Summary: Tips for Healthy Gums
Healthy gums stay pink, firm, and free of bleeding. To keep them that way: brush gently twice daily for two minutes, floss once daily, eat vitamin C– and calcium-rich foods, avoid smoking, and get a professional cleaning every six months. Bleeding, swelling, or recession are early warning signs that shouldn’t be ignored.

Most people take care of their teeth and barely think about their gums — until they bleed, ache, or start pulling away from the tooth. By then, some of the damage is already underway.
Gums aren’t just the pink backdrop for your teeth. They’re a living seal that protects the bone and ligaments holding your teeth in place. Once that seal breaks down, it’s no longer a cosmetic issue — it’s a disease process that, left alone, can cost you teeth.
The encouraging part is that gum disease is one of the most preventable conditions in dentistry, according to organizations like the ADA and CDC. Almost everything that damages gums in the early stage is reversible, and the habits that protect them are simple, cheap, and don’t require a single gadget you don’t already own. This guide — compiled from ADA, CDC, NHS, and Cleveland Clinic patient guidance — walks through what healthy gums actually look like, how to tell when something’s wrong, what genuinely moves the needle at home, and when it’s time to stop self-treating and see a dentist.
Quick Answer
Healthy gums are firm, pink or coral-colored, and never bleed. To keep them that way: brush gently twice a day for two minutes, floss or clean between teeth once a day, eat foods rich in vitamin C and calcium, avoid tobacco, and get a professional cleaning every six months. Mild gingivitis (bleeding, redness, puffiness) usually improves within one to three weeks of consistent care. If bleeding, recession, or looseness persist beyond two weeks, see a dentist — the damage may have progressed past what home care can reverse.
Key Statistics on Gum Health
- Gum disease in some form affects nearly half of adults aged 30 and older in the United States, according to CDC surveillance data (Source 2).
- Severe periodontitis becomes more common with age and is more prevalent among men than women, and among people with lower income and education levels (Source 2).
- Gingivitis, the earliest and fully reversible stage, is estimated to affect a majority of adults at some point, often without them noticing until bleeding appears.
- Smoking remains one of the strongest modifiable risk factors for periodontal disease, and quitting measurably reduces risk over time.
- Gum disease is largely painless in its early and moderate stages, which is why routine dental checks — not symptoms — catch most cases early.
Table of Contents
- What Healthy Gums Look Like
- Healthy Gums vs. Unhealthy Gums
- How Plaque Becomes Tartar
- The Oral Microbiome and Gum Health
- Can Gums Heal Naturally?
- How Long Does Gum Healing Take?
- How to Improve Gum Health Quickly
- How to Make Gums Strong at Home
- Foods That Improve Gum Health
- Daily Gum Care Routine
- Healthy Gum Products
- Risk Factors for Gum Disease, Ranked
- Common Mistakes That Damage Gums
- Special Situations
- My Gums Are Bleeding — What Should I Do?
- Professional Treatment Options
- Home Care vs. Professional Care
- When to Visit a Dentist
- Myths vs. Facts
- Frequently Asked Questions
- Key Takeaways
What Healthy Gums Look Like
Most patients have never actually been told what “normal” gums look like, so they have nothing to compare their own to. Here’s what dentists typically check for in a healthy mouth.
Color: A coral or light pink shade, though this varies with natural pigmentation — people with more melanin often have gums with brown or darker patches, which is completely normal and not a sign of disease.
Firmness: Healthy gum tissue is firm and springs back when you press it gently. It shouldn’t feel spongy or squishy.
Texture: A slightly stippled, orange-peel-like texture on the surface is a good sign in many people — it reflects healthy collagen structure, though its absence alone isn’t automatically a red flag.
Contour: The gum should form a tight, knife-edge collar around each tooth, filling the space between teeth (the papilla) without gaps or puffiness.
Bleeding: None. Healthy gums do not bleed during brushing, flossing, or eating an apple. Bleeding is inflammation, not “just how gums are.”
Smell: No persistent bad breath tied to the gum line. Chronic bad breath is often bacterial and linked to gum inflammation or tongue coating.
Healthy Gums Comparison Table
| Feature | Healthy Gums | Unhealthy Gums |
|---|---|---|
| Color | Coral/light pink (or naturally pigmented) | Red, purplish, or dusky |
| Texture | Firm, slightly stippled | Smooth, shiny, swollen |
| Contour | Tight collar, pointed papilla | Puffy, rolled, or rounded edges |
| Bleeding | None | Bleeds with brushing/flossing |
| Sensitivity | None | Tender or sore to touch |
| Recession | Even gum line | Roots visible, teeth look “longer” |
| Breath | Neutral | Persistent bad breath |
Healthy Gums vs. Unhealthy Gums
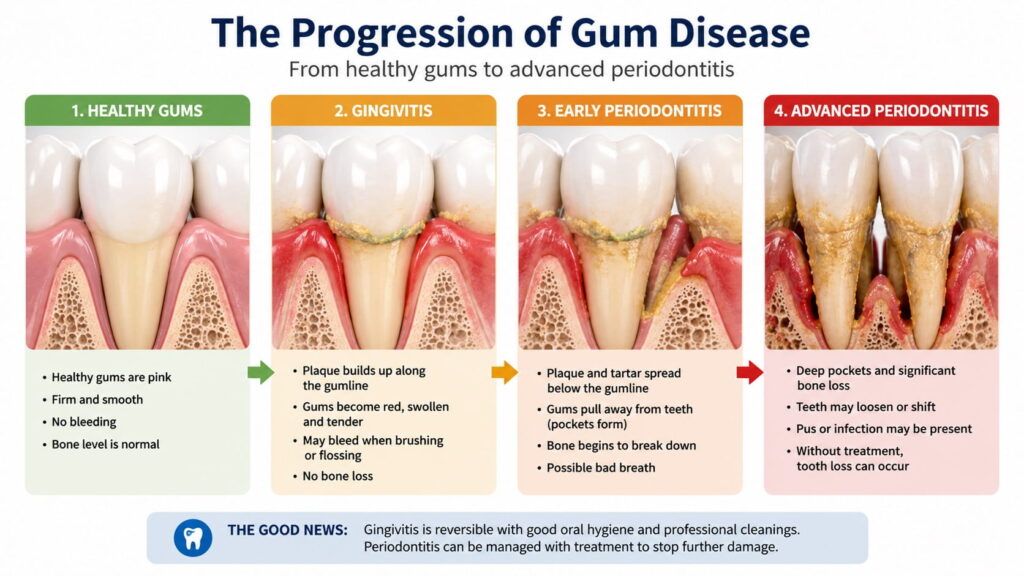
Gum disease doesn’t appear overnight. It moves through recognizable stages, and understanding where you sit on that spectrum changes what you should do next.
Stage 1: Gingivitis (Reversible)
This is inflammation confined to the soft tissue. Plaque bacteria irritate the gum margin, causing redness, puffiness, and bleeding. No bone loss has occurred yet, which is the critical detail — gingivitis is fully reversible with improved oral hygiene and a professional cleaning.
Signs: bleeding gums, mild swelling, redness, tenderness, bad breath.
Stage 2: Early Periodontitis
If gingivitis is ignored, bacteria migrate below the gum line and begin breaking down the fibers and bone that anchor the tooth. Pockets start forming between the tooth and gum. This is no longer purely reversible — it can be controlled and stabilized, but lost bone generally doesn’t regenerate on its own.
Signs: gum recession, slightly loose-feeling teeth, deeper pockets on a dental probe, persistent bad breath.
Stage 3: Moderate to Advanced Periodontitis
Significant bone loss, deeper pockets (often 5mm or more), possible pus, visibly receded gums, and teeth that shift or loosen. This stage requires active periodontal treatment, and in advanced cases, tooth loss becomes a real risk.
Warning Signs Checklist
- Gums bleed when brushing or flossing
- Gums look red, purple, or swollen
- Persistent bad breath or bad taste
- Gums feel tender or sore
- Teeth look longer than they used to (recession)
- Gaps between teeth appear or widen
- Teeth feel loose or shift position
- Pus appears when you press on the gum
- A change in how your bite fits together
If you checked even two or three of these, that’s worth a dental visit, not a wait-and-see approach.
How Plaque Becomes Tartar
Almost every patient has heard the word “tartar” without knowing where it actually comes from — and it’s a genuinely useful thing to understand, because it explains why brushing alone eventually isn’t enough.
Plaque is a soft, sticky biofilm that forms on your teeth within hours of brushing. It’s made of bacteria, food particles, and saliva proteins. At this stage, it’s still soft and can be removed completely with a toothbrush and floss.
The mineralization process: Minerals naturally present in your saliva — mainly calcium and phosphate — gradually seep into that soft plaque layer. Left undisturbed for roughly 24 to 72 hours, plaque begins to harden as these minerals crystallize within it.
Tartar (calculus) is the hardened result. Once plaque has calcified into tartar, it bonds tightly to the tooth surface and, critically, can no longer be removed by brushing or flossing — only professional scaling with dental instruments can take it off.
Why this matters for gum health: tartar has a rough, porous surface that gives fresh plaque bacteria an even easier place to cling to and multiply. It also tends to build up right at the gum line, where it continuously irritates the tissue and drives ongoing inflammation. This is the main reason gingivitis can stall even when someone insists they’re brushing regularly — if tartar has already formed, brushing simply can’t reach the problem anymore.

Expert Tip: If you notice a yellowish or brownish hard deposit near your gum line that doesn’t come off with brushing, that’s very likely tartar, not a stain. It needs a professional cleaning, not a whitening toothpaste.
The Oral Microbiome and Gum Health
This is one of the more genuinely interesting shifts in how dentistry thinks about gum disease, and it rarely gets mentioned in consumer-facing articles.
Your mouth hosts hundreds of bacterial species living in a relatively stable community called the oral microbiome. In a healthy mouth, this community is dominated by species that coexist peacefully with your gum tissue. Gum disease isn’t simply caused by “too much bacteria” — it’s more accurately described as a shift in the balance of that community, sometimes called dysbiosis.
When plaque is allowed to accumulate undisturbed, the environment beneath the gum line becomes low in oxygen. That shift favors a different set of bacteria — anaerobic species that are far more inflammatory and destructive to gum tissue than the bacteria that dominate a healthy mouth. Certain species associated with this shift, along with a few “keystone” bacteria that disproportionately disrupt the balance even in small numbers, are strongly linked to the transition from gingivitis to periodontitis.
This matters practically for two reasons. First, it explains why mechanical plaque removal (brushing, flossing, professional cleaning) works: it physically disrupts the biofilm before it can mature into a more harmful community, rather than simply “killing germs.” Second, it explains why some people develop aggressive gum disease despite decent hygiene, and others get away with mediocre hygiene for years — individual immune response and microbiome composition both play a role, alongside genetics.
Emerging research into probiotics for oral health (certain Lactobacillus and Streptococcus strains) is exploring whether reintroducing “friendly” bacteria can help rebalance the microbiome, but the evidence is still preliminary and this shouldn’t be treated as a substitute for mechanical cleaning and professional care.
Can Gums Heal Naturally?
This is one of the most common questions I get, and the honest answer depends entirely on which stage you’re in.
If you have gingivitis (inflammation only, no bone loss): Yes. Gum tissue in this stage can fully heal on its own once the irritant — plaque and, if present, tartar — is consistently removed. This is genuinely “natural” healing in the sense that your body’s own repair processes do the work; your job is just to stop reinjuring the tissue every day.
If you have periodontitis (bone and attachment loss has occurred): No, not fully. The bone and connective fibers that anchored the tooth do not regenerate on their own once lost. Treatment can stop the disease from progressing and, in some cases, regenerative procedures (like bone grafting) can rebuild some lost support — but this requires professional intervention, not home care alone.
What “natural” methods can and can’t do: Diet, hydration, stress management, and good hygiene all genuinely support the tissue’s own healing capacity — that part is real and evidence-based. What isn’t supported by evidence is the idea that any oil, herb, or rinse can dissolve tartar, regenerate lost bone, or “cure” periodontitis without professional treatment. Be skeptical of any product claiming to do so.
How Long Does Gum Healing Take?
This is one of the most common questions people ask before a wedding, a job interview, or a dental check-up they’ve been avoiding. The honest answer: some improvement happens fast, some doesn’t.
| Condition | Realistic Healing Timeline | What’s Required |
|---|---|---|
| Mild gingivitis (bleeding, redness) | 3–10 days for bleeding to reduce; 1–2 weeks for full resolution | Consistent brushing + flossing |
| Gingivitis with tartar present | 1–3 weeks after professional cleaning | Scaling + home care |
| Gum swelling after a deep cleaning | 1–2 weeks | Gentle rinsing, good hygiene, follow-up as advised |
| Early periodontitis pockets | Weeks to months to stabilize; depth reduction varies | Scaling and root planing, improved home care |
| Gum recession | Does not reverse naturally | Gum graft if significant and symptomatic |
| Bone loss from periodontitis | Does not regenerate without surgery | Regenerative periodontal surgery in select cases |
Most patients with simple gingivitis notice less bleeding within a week and calmer, less puffy gums within two to three weeks. If nothing has improved after three to four weeks of genuinely consistent care, that’s a sign you need professional periodontal evaluation rather than more home effort — tartar or a deeper pocket is likely present.
How to Improve Gum Health Quickly
What Can Improve in Days
Mild gingivitis often responds within 3 to 10 days of consistent, correct brushing and flossing. Bleeding tends to decrease first — that’s the surface inflammation calming down. Swelling and color often follow over the following one to two weeks.
What Takes Longer
Gum tissue that has already receded will not regrow at home. Pocket depth from periodontitis narrows slowly, if at all, without professional scaling. Bone that’s already been lost stays lost unless a specialist performs regenerative treatment.
Myths vs. Facts on Quick Fixes
| Myth | Fact |
|---|---|
| Brushing harder makes gums healthier faster | Aggressive brushing causes recession and doesn’t remove more plaque |
| Mouthwash alone can reverse gum disease | Mouthwash supports a routine but can’t replace mechanical plaque removal |
| Oil pulling cures gingivitis | Some small studies show modest plaque reduction, but evidence is weak; it’s not a substitute for brushing and flossing |
| Gum disease can’t be sped up in recovery | A professional cleaning combined with home care meaningfully accelerates healing compared to home care alone |
The Fastest Realistic Plan
- Book a professional cleaning to remove hardened tartar that a toothbrush cannot touch.
- Brush twice daily for two full minutes with a soft-bristled or electric brush.
- Floss or use interdental brushes once daily, reaching below the gum line gently.
- Add an antimicrobial or fluoride mouthwash if your dentist recommends one for your specific case.
- Cut back on smoking and sugary drinks during the recovery window — both actively slow healing.
How to Make Gums Strong at Home
“Strong” gums really means well-supported, non-inflamed tissue sitting on stable bone. Here’s what actually contributes to that.
Brushing Technique
Use a soft-bristled or electric toothbrush, angle the bristles at roughly 45 degrees toward the gum line, and use short, gentle strokes rather than a hard back-and-forth scrub. Brush for two full minutes, twice a day, consistent with general ADA recommendations for brushing twice daily with fluoride toothpaste for two minutes (Source 1). Aggressive scrubbing is one of the most common ways patients unintentionally injure their own gums.
Flossing and Interdental Cleaning
Floss reaches tooth surface a brush can’t touch. Professional cleaning, tooth brushing, and cleaning between teeth using floss or tools like interdental brushes have been shown to disrupt and remove plaque (Source 1). Curve the floss into a “C” shape around each tooth and slide it gently below the gum line rather than snapping it in. If traditional floss is difficult, interdental brushes or a water flosser are legitimate alternatives.
Tongue Cleaning
The tongue harbors bacteria that contribute to bad breath and can reseed the gum line with plaque-forming bacteria. A tongue scraper or the brush on the back of most toothbrush heads takes about 10 seconds and is worth adding to your morning routine.
Mouthwash
An antimicrobial mouthwash can reduce plaque and gingivitis when used alongside brushing and flossing — not instead of them. Alcohol-based rinses can dry the mouth and irritate tissue in some people, so an alcohol-free formula is often gentler for sensitive gums.
Hydration
Saliva is one of the gums’ natural defenses — it buffers acid and washes away debris. Chronic dry mouth (xerostomia), whether from dehydration, mouth breathing, or medication side effects, is strongly linked to higher plaque buildup and gum irritation.
Smoking and Vaping Cessation
Tobacco use is one of the single strongest risk factors for periodontal disease. Nicotine constricts blood vessels in the gums, which masks bleeding (a warning sign smokers often don’t see) while still allowing disease to progress underneath. Vaping is not risk-free either; nicotine and vapor chemicals still affect gum blood flow and healing.
Stress Reduction
Chronic stress raises cortisol, which can suppress immune response and has been associated with more severe gum inflammation, plus stress-related habits like teeth grinding that put extra load on the gum and bone.
Sleep
Poor sleep is linked with weaker immune function generally, and there’s a documented association between insufficient sleep and higher rates of gum disease, likely through the same inflammatory and immune pathways.
Diabetes Management
Blood sugar and gum health run in both directions: uncontrolled diabetes makes gum disease more likely and more severe, and untreated gum disease can make blood sugar harder to control. If you have diabetes, this isn’t a minor detail — it’s a core part of your dental care plan.
Tip: If you have diabetes, mention your most recent HbA1c to your dentist — it changes how closely your gums should be monitored.
Foods That Improve Gum Health

Nutrients That Support Gum Tissue
Vitamin C is essential for collagen production, the structural protein that holds gum tissue together. Deficiency is directly linked to bleeding, swollen gums. Good sources: citrus fruits, bell peppers, strawberries, kiwi, broccoli.
Vitamin D supports calcium absorption and has anti-inflammatory properties; low vitamin D levels have been associated with a higher risk of periodontal disease in several studies. Sources: fatty fish, egg yolks, fortified dairy, sensible sun exposure.
Calcium supports the jawbone that anchors your teeth. Sources: dairy, leafy greens, almonds, fortified plant milks.
Omega-3 fatty acids have anti-inflammatory effects that some research links to reduced gum disease severity. Sources: salmon, mackerel, walnuts, flaxseed.
Leafy greens (spinach, kale) supply folate and vitamin K, both involved in tissue repair and healthy blood clotting at the gum line.
Crunchy vegetables like carrots and celery mechanically stimulate saliva flow and gently help clear surface debris, though they are not a substitute for brushing.
Berries and citrus bring antioxidants and vitamin C that combat the oxidative stress associated with chronic gum inflammation.
Green tea contains catechins, plant compounds studied for their ability to reduce inflammatory markers and inhibit some plaque-forming bacteria.
Foods and Habits That Worsen Gum Health
- Sugary and starchy foods feed the bacteria that produce plaque acid. Nutrient-rich foods like leafy greens, dairy, and lean proteins support strong teeth and gums, while limiting sugary snacks and drinks reduces risk.
- Sticky, refined carbohydrates (candy, white bread, chips) linger on the gum line longer than most foods.
- Frequent sipping on sugary or acidic drinks keeps the mouth in an acidic state for hours rather than minutes.
- Alcohol in excess dries the mouth and reduces saliva’s protective effect.
Foods for Gum Health at a Glance
| Nutrient | Why It Matters | Good Sources |
|---|---|---|
| Vitamin C | Collagen production, tissue repair | Citrus, bell peppers, strawberries |
| Vitamin D | Anti-inflammatory, calcium absorption | Fatty fish, fortified dairy, sunlight |
| Calcium | Jawbone density | Dairy, leafy greens, almonds |
| Omega-3 | Reduces gum inflammation | Salmon, walnuts, flaxseed |
| Antioxidants | Combat oxidative stress | Berries, green tea, leafy greens |
| Fiber/crunch | Mechanical cleaning, saliva stimulation | Carrots, celery, apples |
Daily Gum Care Routine
Morning Routine
- Brush for two minutes with fluoride toothpaste, gentle circular or short strokes.
- Floss or use an interdental brush.
- Rinse with mouthwash if recommended for your case.
- Clean your tongue.
Night Routine
- Floss before brushing at night — this loosens debris the toothbrush can then clear.
- Brush for two minutes, paying attention to the gum line, not just the tooth surface.
- Avoid eating or drinking anything except water afterward.
Weekly Habits
- Check your gums in the mirror for color, swelling, or recession changes.
- Replace your toothbrush head if bristles look frayed (roughly every 3 months regardless of appearance).
- Reassess snacking habits if you’ve been grazing on sugary foods.
Professional Cleanings
Most people benefit from a professional cleaning and check-up every six months, though people with a history of gum disease, smoking, or diabetes often need a three-to-four-month interval instead.
Healthy Gum Products
Toothbrushes: A soft-bristled manual brush with a small head reaches awkward areas better than a large, stiff-bristled one.
Electric toothbrushes: Oscillating-rotating or sonic electric brushes have been shown in multiple studies to remove more plaque and reduce gingivitis more than manual brushing, largely because they make consistent, correct technique easier to maintain.
Toothpaste: Look for fluoride as the active ingredient. Some formulas add stannous fluoride or other antibacterial agents specifically marketed for gum health.
Floss: Waxed, unwaxed, or floss picks all work if used correctly and daily.
Interdental brushes: Small bottle-brush-shaped tools that clean between teeth, especially useful for people with larger gaps, braces, or bridges.
Water flossers: Effective at flushing debris and reducing bleeding, particularly helpful for people with braces, implants, or limited hand dexterity.
Mouthwash: Antimicrobial or fluoride rinses can be a useful addition, particularly for people prone to gingivitis.
Note: Look for the ADA Seal of Acceptance on oral care products where available — it indicates the product has been evaluated for safety and efficacy claims.
Risk Factors for Gum Disease, Ranked
Not all risk factors carry equal weight. Here’s roughly how dentists rank them by clinical impact, based on how consistently they show up in patients with more severe disease.
| Rank | Risk Factor | Impact Level | Modifiable? |
|---|---|---|---|
| 1 | Smoking/tobacco use | Very high | Yes |
| 2 | Poor oral hygiene (plaque/tartar buildup) | Very high | Yes |
| 3 | Uncontrolled diabetes | High | Partially |
| 4 | Genetics/family history | High | No |
| 5 | Age | Moderate–high | No |
| 6 | Certain medications (causing dry mouth or gum overgrowth) | Moderate | Partially |
| 7 | Hormonal changes (pregnancy, menopause) | Moderate | No |
| 8 | Chronic stress | Moderate | Yes |
| 9 | Poor nutrition | Moderate | Yes |
| 10 | Crooked teeth or ill-fitting dental work | Low–moderate | Partially |
| 11 | Immune-suppressing conditions | Moderate–high | Partially |
Common Mistakes That Damage Gums
- Brushing too hard — one of the most common causes of gum recession dentists report.
- Skipping flossing — brushing alone misses nearly half the tooth surface.
- Using a hard-bristled brush — feels “thorough” but abrades gum tissue over time.
- Ignoring bleeding gums — treating bleeding as normal instead of as the early warning sign it actually is.
- Not replacing your toothbrush — worn bristles clean poorly and can harbor bacteria.
- Smoking or vaping — masks symptoms while disease progresses.
- Skipping dental check-ups — tartar cannot be removed at home once it hardens.
- Constant snacking — keeps your mouth in an acidic, plaque-friendly state all day.
- Mouth breathing at night — dries tissue and increases plaque accumulation.
Special Situations
Pregnancy and Gum Health
Hormonal changes during pregnancy increase blood flow to gum tissue and exaggerate the inflammatory response to plaque, a pattern often called “pregnancy gingivitis.” It’s common, manageable with more frequent professional cleanings and diligent home care, and it’s safe — and advisable — to continue routine dental visits during pregnancy.
Diabetes and Gums
This relationship runs both directions. Diabetic patients should treat gum checks as part of routine diabetes management, not a separate concern.
Aging and Gums
Gum recession becomes more common with age, partly from decades of cumulative wear and partly from thinner tissue. Root surfaces that become exposed are more prone to decay and sensitivity.
Braces and Gum Care
Orthodontic brackets trap plaque in new places. Interdental brushes, orthodontic floss threaders, and water flossers become essential rather than optional during treatment.
Children’s Gum Health
Gingivitis can appear in children, usually tied to inconsistent brushing rather than disease risk factors seen in adults. Supervising brushing until a child has the coordination to do it thoroughly (often around age 7–8) meaningfully reduces this.
Medications That Affect Gums
Certain medications — some blood pressure drugs (calcium channel blockers), anti-seizure medications (phenytoin), and immunosuppressants (cyclosporine) — can cause gum overgrowth. Other medications cause dry mouth, indirectly raising gum disease risk. Always mention your full medication list to your dentist.
My Gums Are Bleeding — What Should I Do?
Use this simple decision path to figure out your next step.
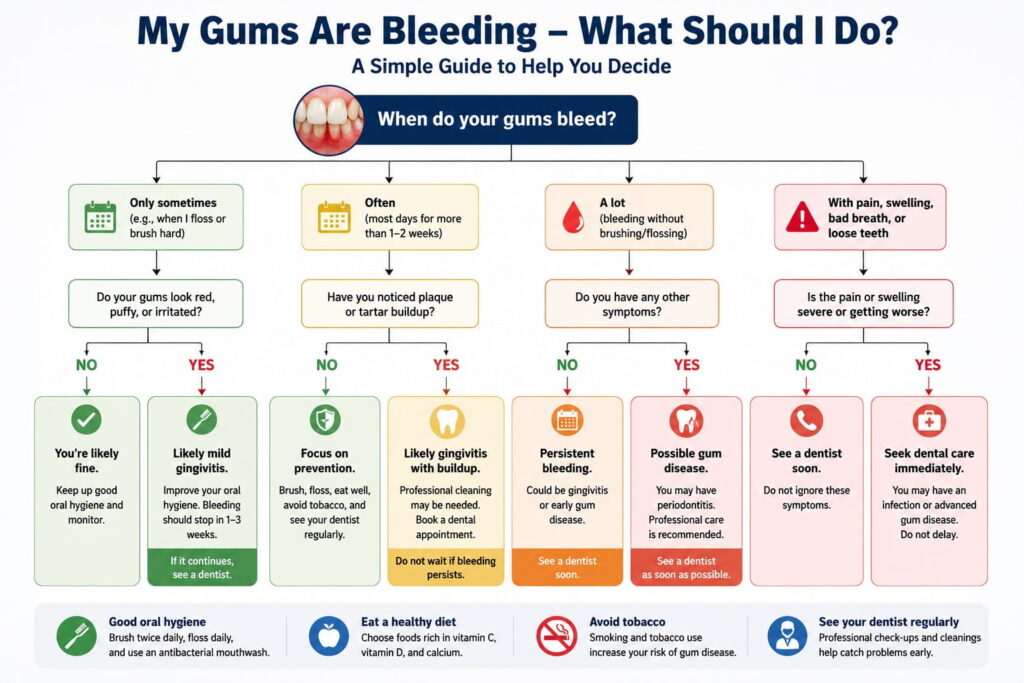
Are your gums bleeding?
│
├─ NO → Maintain your current routine. Recheck in 6 months.
│
└─ YES
│
├─ Is it isolated to one spot after aggressive brushing/flossing?
│ └─ YES → Switch to a soft brush and gentler technique.
│ Reassess in 3–5 days.
│
└─ Is it happening across multiple teeth, most days?
│
├─ Has it lasted less than 2 weeks?
│ └─ Improve brushing/flossing consistency.
│ Recheck in 1–2 weeks.
│
└─ Has it lasted more than 2 weeks despite good hygiene?
└─ See a dentist. Tartar buildup or early
periodontitis is likely — professional
cleaning is needed, not more brushing.
Additional red flags that mean “see a dentist now” regardless of duration: pus at the gum line, loose teeth, visible recession, or a change in your bite.
Professional Treatment Options
Home care resolves gingivitis, but once disease has progressed, professional treatment becomes necessary. Here’s what that typically looks like, from least to most invasive.
Scaling and root planing (deep cleaning): The standard first-line treatment for periodontitis. A hygienist or dentist removes tartar and bacterial deposits from below the gum line and smooths the root surface to help gum tissue reattach. Often done under local anesthesia over one or two visits.
Antibiotic therapy: Localized antibiotic gels or, in some cases, oral antibiotics may be used alongside scaling for more aggressive or persistent infections. This supplements, rather than replaces, mechanical cleaning.
Laser therapy: Some practices use laser-assisted procedures to remove diseased tissue and reduce bacteria with less bleeding and discomfort than traditional surgery. Evidence supports it as an adjunct in select cases, though it isn’t a universal substitute for scaling and root planing.
Periodontal (flap) surgery: For deeper pockets that don’t respond to non-surgical treatment, a periodontist folds back the gum tissue to access and clean the root surface and underlying bone directly, then sutures the tissue back into a healthier position.
Bone or tissue grafting: Used to rebuild bone or gum tissue lost to periodontitis, particularly around specific teeth at risk of loss. This is regenerative treatment, not a routine procedure.
Gum grafting for recession: Tissue taken from elsewhere in the mouth (or a donor source) is used to cover exposed roots and restore a natural gum line, primarily addressing sensitivity and appearance.
Maintenance therapy: After active treatment, patients typically move to more frequent professional cleanings (often every 3–4 months) to keep the disease from returning.
Home Care vs. Professional Care
| Situation | Home Care Alone | Needs Professional Treatment |
|---|---|---|
| Mild bleeding, no tartar visible | Usually sufficient | — |
| Bleeding persisting beyond 2 weeks | Not sufficient | Yes — likely tartar buildup |
| Visible hard yellow/brown deposit at gum line | Not sufficient (cannot be brushed off) | Yes — professional scaling required |
| Gum recession | Cannot reverse it | Yes, if significant or symptomatic |
| Loose or shifting teeth | Not sufficient | Yes, urgently |
| Pus at the gum line | Not sufficient | Yes, urgently |
| Deep pockets (measured by a dentist) | Not sufficient | Yes — scaling and root planing |
| General plaque prevention/maintenance | Sufficient | Routine 6-month checks still recommended |
When to Visit a Dentist
See a dentist within the next couple of weeks if you notice:
- Bleeding that doesn’t improve after 1–2 weeks of better home care
- Persistent swelling, redness, or tenderness
- Gum recession or teeth that look longer
- Loose or shifting teeth
- Pus at the gum line
- Persistent bad breath despite good hygiene
- A change in how your teeth fit together when biting
Don’t wait for pain. Gum disease is frequently painless until it’s advanced — that’s exactly why routine six-month checks catch problems people can’t feel yet.
Myths vs. Facts
| Myth | Fact |
|---|---|
| Bleeding gums are normal if you brush regularly | Bleeding always signals inflammation and should be addressed, not ignored |
| Harder brushing cleans better | Hard brushing causes recession and doesn’t remove more plaque than gentle brushing |
| Gum disease only affects older adults | Gingivitis can start in the teens and twenties |
| If it doesn’t hurt, it’s fine | Gum disease is often painless until advanced stages |
| Whitening toothpaste improves gum health | Whitening toothpaste targets stains, not gum tissue |
| Mouthwash replaces brushing | Mouthwash supports but cannot replace mechanical plaque removal |
| Natural remedies alone can cure gum disease | Some (like green tea) support gum health, but none reverse periodontitis without professional care |
| Once tartar forms, brushing harder removes it | Only professional scaling removes calcified tartar |
Frequently Asked Questions
1. What do healthy gums look like?
Firm, coral or light pink (allowing for natural pigmentation), tightly hugging each tooth, with no bleeding, swelling, or persistent bad breath.
2. Can gum disease be reversed?
Gingivitis, the early stage, is fully reversible with better oral hygiene and professional cleaning. Periodontitis, which involves bone loss, can be controlled and stabilized but generally isn’t fully reversible.
3. Can gums heal naturally without a dentist?
Yes, if it’s gingivitis without bone loss — your body can fully heal that tissue once plaque is consistently removed. Periodontitis requires professional treatment to stop progression.
4. Why do my gums bleed when I brush or floss?
Bleeding usually indicates gum inflammation from plaque buildup, called gingivitis. It’s a sign to clean more thoroughly and consistently, then see a dentist if it persists.
5. How can I improve my gum health quickly?
Consistent, gentle brushing twice daily, daily flossing, and a professional cleaning to remove hardened tartar produce the fastest realistic improvement, often within one to three weeks for mild gingivitis.
6. How long does it take for gums to heal after a deep cleaning?
Most people see reduced swelling and bleeding within one to two weeks, though full tissue reattachment and pocket reduction can take several weeks to months.
7. What foods are good for gum health?
Vitamin C–rich fruits and vegetables, dairy and leafy greens for calcium, fatty fish for omega-3s, and crunchy vegetables that stimulate saliva all support healthier gums.
8. What foods are bad for gums?
Sugary snacks, sticky refined carbohydrates, and frequent sipping on sugary or acidic drinks feed plaque bacteria and worsen inflammation.
9. How often should I floss?
Once daily is the standard recommendation, ideally before brushing so loosened debris can be brushed away.
10. Is an electric toothbrush better for gum health?
Studies generally show electric brushes, particularly oscillating-rotating designs, remove more plaque and reduce gingivitis more than manual brushing over time.
11. What is the best mouthwash for gum health?
An antimicrobial or fluoride mouthwash used alongside brushing and flossing can help reduce plaque and gingivitis; alcohol-free formulas are often gentler for sensitive or inflamed gums.
12. Can stress cause gum disease?
Chronic stress can suppress immune response and has been linked to more severe gum inflammation, plus stress-related grinding that strains gum and bone tissue.
13. Does smoking really affect gum health that much?
Yes, smoking is one of the strongest risk factors for periodontal disease and also masks bleeding, a key early warning sign, delaying diagnosis.
14. What are the first signs of gum disease?
Bleeding during brushing or flossing, redness, mild swelling, and bad breath are typically the earliest signs.
15. Can gum recession grow back?
No — receded gum tissue does not regenerate naturally. A gum graft can address significant recession, but prevention is more effective than reversal.
16. Is gum disease linked to other health conditions?
Yes — research has linked periodontal disease to diabetes, cardiovascular disease, and adverse pregnancy outcomes, though the exact causal mechanisms are still being studied.
17. How do I know if I have gingivitis or periodontitis?
Gingivitis involves inflammation without bone loss and no gum detachment from the tooth. Periodontitis involves measurable pocket depth and bone loss, which only a dentist can assess with a probe and X-rays.
18. Can children get gum disease?
Children can develop gingivitis, usually linked to inconsistent brushing rather than the deeper risk factors seen in adults.
19. Should I use a water flosser instead of regular floss?
A water flosser is a good alternative or supplement, especially for braces or limited dexterity, but traditional floss or interdental brushes remain effective for most people when used correctly.
20. What is scaling and root planing?
It’s a non-surgical deep cleaning that removes tartar and bacteria from below the gum line and smooths root surfaces, typically the first treatment for periodontitis.
21. Does mouthwash kill the bacteria that cause gum disease?
Antimicrobial mouthwash can reduce bacterial load and plaque, but it works as a supplement to brushing and flossing, not a replacement, since it can’t physically disrupt biofilm the way brushing does.
22. Why do my gums hurt but not bleed?
Soreness without bleeding can result from aggressive brushing, a new dental appliance, teeth grinding, or a localized irritation; if it persists beyond a week, a dentist should evaluate it.
23. Is bad breath always a sign of gum disease?
Not always — diet, dry mouth, and tongue coating also cause bad breath — but persistent bad breath despite good hygiene is common in gum disease and worth having checked.
Key Takeaways
- Healthy gums are firm, pink (allowing for natural pigmentation), and never bleed.
- Bleeding, swelling, or persistent bad breath are early warning signs, not normal variation.
- Gingivitis is reversible; periodontitis (bone loss) is manageable but not fully reversible.
- Once plaque hardens into tartar, only professional scaling can remove it — brushing can’t.
- Brushing twice daily, flossing once daily, and six-month professional cleanings form the foundation of gum health.
- Diet, smoking, sleep, stress, and conditions like diabetes all measurably affect gum health.
- See a dentist promptly if bleeding persists beyond one to two weeks of improved home care, or if you notice recession, looseness, or pus.
Sources
- American Dental Association — Home Oral Care
- CDC — Oral Health Prevention Tips for Adults
- NHS — Take Care of Your Teeth and Gums